
Latest News
 Legally required expense records still missing for several current, former NH officials
Legally required expense records still missing for several current, former NH officials
 Community health workers, Republicans disagree over who should pay for their services
Community health workers, Republicans disagree over who should pay for their services
 Granite Geek: Free government software for taxes – what could go wrong? (Not much, as it turns out)
Granite Geek: Free government software for taxes – what could go wrong? (Not much, as it turns out)
 Opinion: The inspiring life of Howard Zinn
Opinion: The inspiring life of Howard Zinn
 High schools: Friday and Saturday results
High schools: Friday and Saturday results
 To snuff out cancer, NH firefighters seek regular screenings
To snuff out cancer, NH firefighters seek regular screenings
 Recycled Percussion to perform free concert for first responders at Flying Monkey
Recycled Percussion to perform free concert for first responders at Flying Monkey

Steeplegate project to reopen to public comment as developer seeks to reduce required parking
The developer looking to turn the mostly vacant Steeplegate Mall into a bustling mix of residences and retail is seeking relief from the city’s minimum parking requirements to reduce the amount of pavement at the massive redevelopment project.The...

Students and staff welcome the opening of new Allenstown K-8 school
Five years after planning for a new school building in Allenstown began and 19 months after builders broke ground at 171 River Road, the Allenstown Community School opened on Friday.The big day was celebrated with white shirts emblazoned with...
Most Read
 Steeplegate project to reopen to public comment as developer seeks to reduce required parking
Steeplegate project to reopen to public comment as developer seeks to reduce required parking
 A turbulent 50-year history: Inside the rise and fall of a tiny Catholic college in Warner
A turbulent 50-year history: Inside the rise and fall of a tiny Catholic college in Warner
 Students and staff welcome the opening of new Allenstown K-8 school
High schools: Friday and Saturday results
Students and staff welcome the opening of new Allenstown K-8 school
High schools: Friday and Saturday results
 Hopkinton chocolatier transforms chocolates into works of art
Hopkinton chocolatier transforms chocolates into works of art
 School Board to vote on new Broken Ground principal nominee
School Board to vote on new Broken Ground principal nominee
Editors Picks
A turbulent 50-year history: Inside the rise and fall of a tiny Catholic college in Warner
 In Warner, housing committee driving conversation on new solutions
In Warner, housing committee driving conversation on new solutions
 The murky world of town and city flags in NH
Hopkinton chocolatier transforms chocolates into works of art
The murky world of town and city flags in NH
Hopkinton chocolatier transforms chocolates into works of art

Sports

Softball: Cassidy Emerson may have eight freshmen on her team, but the Falcons have glided to an 8-1 start
BOW — Taking over a program with eight incoming freshmen sounded daunting to Cassidy Emerson as she geared up for her first season as the new Bow softball head coach. After Friday’s 9-0 win over Pelham (3-5), though, the Falcons are now 8-1, right...
 High schools: Hopkinton lax sweeps opponents, more Thursday results
High schools: Hopkinton lax sweeps opponents, more Thursday results
 Celtics turn off Heat; Cavs or Magic on deck
Celtics turn off Heat; Cavs or Magic on deck
 Baseball: Merrimack Valley now 6-1 following wild game at Pembroke Academy
Baseball: Merrimack Valley now 6-1 following wild game at Pembroke Academy
 High schools: Wednesday’s baseball, softball, lacrosse and tennis results
High schools: Wednesday’s baseball, softball, lacrosse and tennis results
Opinion

Opinion: Seeking wisdom in literature
Gib West lives in Concord. Many pieces of great literature explore the themes of power and hubris, and thus can be revisited to examine how we, as members of a community, can question ourselves or our leaders and in so doing seek a just path.It is...
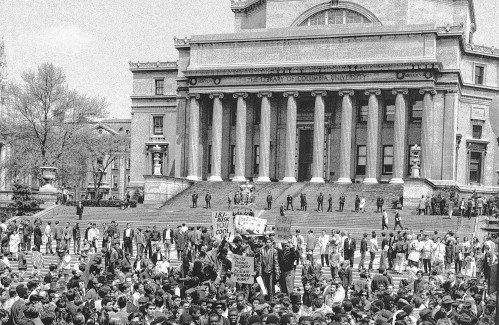 Opinion: It all started at Columbia
Opinion: It all started at Columbia
 Opinion: Students resist: Berkeley to Gaza, Columbia to Jenin, UNH to Rafah
Opinion: Students resist: Berkeley to Gaza, Columbia to Jenin, UNH to Rafah
 Opinion: New Hampshire, it’s time to acknowledge the stories of suffering
Opinion: New Hampshire, it’s time to acknowledge the stories of suffering
 Opinion: A digital equity plan for Granite Staters
Opinion: A digital equity plan for Granite Staters

Politics

House passes bill to raise minimum marriage age to 18, sending it to governor
The New Hampshire House passed a bill Thursday raising the legal age of marriage to 18, sending the legislation to Gov. Chris Sununu’s desk after years of advocacy.Senate Bill 359, which passed 192-174, states that “no person below the age of 18 years...
 Charities will not have to pay rent to casinos under new law
Charities will not have to pay rent to casinos under new law
 Sununu says he’ll support Trump even if he’s convicted
Sununu says he’ll support Trump even if he’s convicted
 NH mayors want more help from state on homelessness prevention funds
NH mayors want more help from state on homelessness prevention funds
 Two democrats with parallel views run for same State Senate seat
Two democrats with parallel views run for same State Senate seat
e-Edition
Arts & Life

From the Farm: Think like a cow
Do you ever wonder how your dog thinks? It’s usually easy to read your dog’s mind: “I want to go out,” “I’m hungry (always),” “I love you.” How about your cat? She’s more like, “Leave me alone,” “Scratch my belly,” “Leave me alone. I mean it. Leave....
 Take Me Outside: Lights out for wildlife
Take Me Outside: Lights out for wildlife
 Vintage Views: The Simple Genius – John Clark
Vintage Views: The Simple Genius – John Clark
 PILLAR Gallery + Projects opens fourth exhibition in Concord
PILLAR Gallery + Projects opens fourth exhibition in Concord
 Concord Community Music School presents Bach’s Lunch: Hildaland
Concord Community Music School presents Bach’s Lunch: Hildaland
Obituaries
 Miriam Chamberlin
Miriam Chamberlin
Concord, NH - Miriam Helen (Gaskell) Chamberlin, 92, passed away Saturday April 20, 2024 at Pleasant View Center nursing home, Concord, NH, after a long period of failing health. She was born in Concord, NH on February 25, 1932, the dau... remainder of obit for Miriam Chamberlin
 Junie Landry
Junie Landry
Mesa, AZ - Junie L. Landry, 93, passed away after a sudden illness on Tuesday, April 9, 2024. She was born in May, 1930 in Laconia, NH, to Harry S. and Thelma I. (Trumbull) Waite. She attended Laconia High School while living at 56... remainder of obit for Junie Landry
 Sandra Scheys
Sandra Scheys
Bow, NH - Sandra Renee Scheys, age 60, died on Tuesday, April 16th, 2024 at St. Vincent's Hospital in Worcester, MA, after a short battle with cancer. Born on July 22, 1963 in Concord, Sandie attended schools in Bow, NH and Bishop B... remainder of obit for Sandra Scheys
 Joseph M. Jenovese Jr.
Joseph M. Jenovese Jr.
Concord, NH - Joseph M. Jenovese Jr., age 88, of Eastside Drive, Concord, passed away peacefully at his home on Sunday, April, 28th 2024, surrounded by his family, following a period of declining health. He was born on November 11th, 19... remainder of obit for Joseph M. Jenovese Jr.

