
Latest News
 Baseball: Bow secures top-four seed with win over Kingswood
Baseball: Bow secures top-four seed with win over Kingswood
 High schools: Concord boys’ lax secures tourney spot with victory, Kearsarge and Brady tennis advance to semis, more results from Thursday
High schools: Concord boys’ lax secures tourney spot with victory, Kearsarge and Brady tennis advance to semis, more results from Thursday
 Stefany Shaheen, daughter of New Hampshire senator, launches House bid
Stefany Shaheen, daughter of New Hampshire senator, launches House bid
 Senate lawmakers vote to lift betting limits to attract high-rollers to New Hampshire’s casinos
Senate lawmakers vote to lift betting limits to attract high-rollers to New Hampshire’s casinos
 Two Villages Art Society begins summer members show
Two Villages Art Society begins summer members show
 High schools: Bow girls’ tennis advances in tourney, Stark baseball beats MV, Kearsarge softball wins first games of the season; Wednesday’s results
High schools: Bow girls’ tennis advances in tourney, Stark baseball beats MV, Kearsarge softball wins first games of the season; Wednesday’s results

Georgia’s Northside in Concord transitions into catering and cooking classes
Beyond raising his two kids, Alan Natkiel, owner of Georgia’s Northside Southern Kitchen & Beer Market, considers the dedication and love he puts into his Concord establishment as equal to caring for a third child.

‘You have time’ – Coe-Brown graduates savor the moment
He may have been a year behind her in school, but Kayleigh Hollis looks up to her younger brother, Kaiden.
Most Read
 ‘Bittersweet’: The Post on Main Street closes Friday
‘Bittersweet’: The Post on Main Street closes Friday
 Messy parking around Concord’s bus terminal won’t get less messy any time soon
Messy parking around Concord’s bus terminal won’t get less messy any time soon
 Jesse Sullivan pleads guilty to second-degree murder of half-brother, Zackary
Jesse Sullivan pleads guilty to second-degree murder of half-brother, Zackary
 In echo of 2014 struggle, Market Basket board sidelines ‘Artie T.’ from CEO spot
In echo of 2014 struggle, Market Basket board sidelines ‘Artie T.’ from CEO spot
 Historic former Boscawen library building on sale – again
Historic former Boscawen library building on sale – again
 New Concord apartments open in former First Congregational Church
New Concord apartments open in former First Congregational Church
Editors Picks
 The Monitor’s guide to the New Hampshire legislature
The Monitor’s guide to the New Hampshire legislature
 One year after UNH protest, new police body camera footage casts doubt on assault charges against students
One year after UNH protest, new police body camera footage casts doubt on assault charges against students
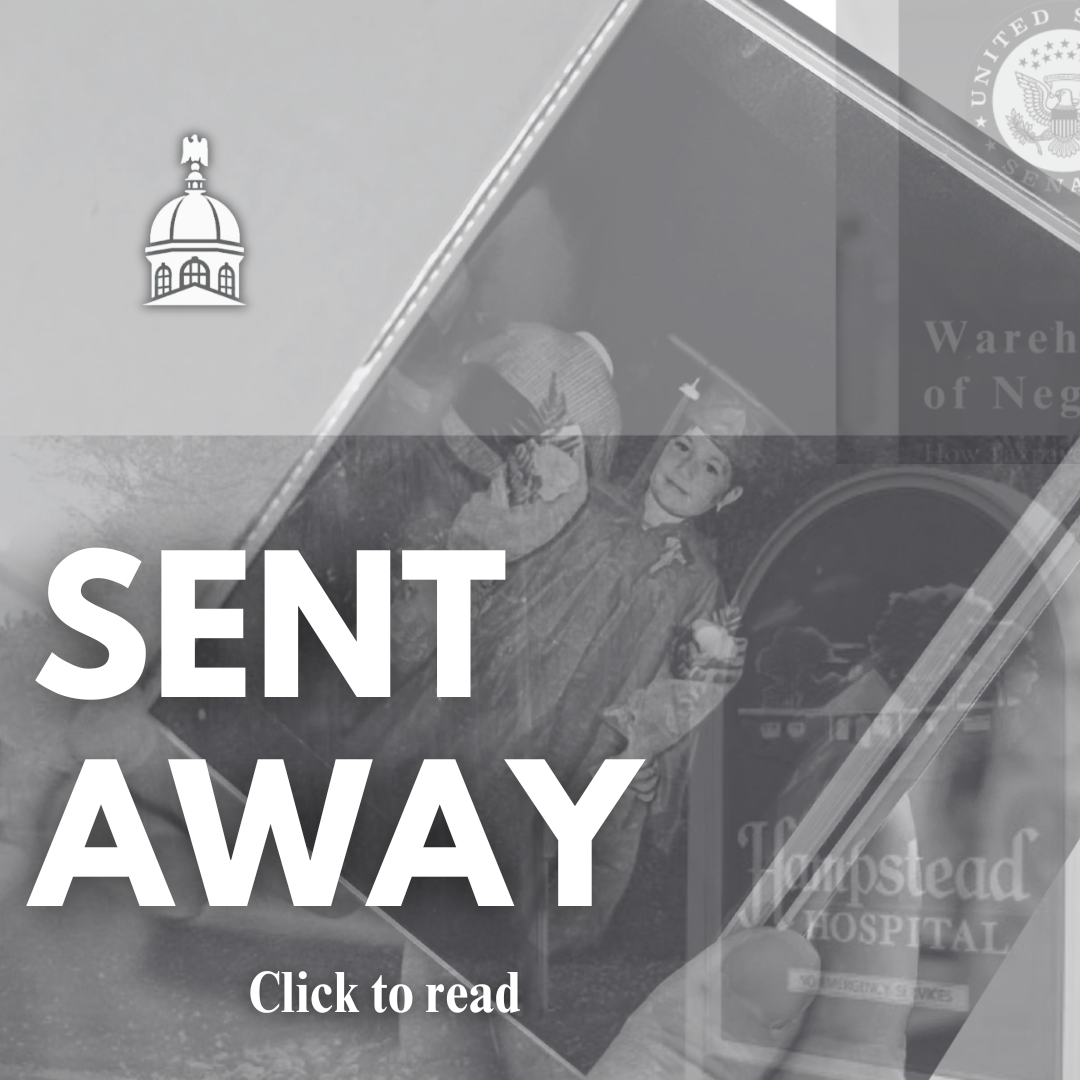
 ‘It’s always there’: 50 years after Vietnam War’s end, a Concord veteran recalls his work to honor those who fought
‘It’s always there’: 50 years after Vietnam War’s end, a Concord veteran recalls his work to honor those who fought
 ‘We honor your death’ – Arranging services for those who die while homeless in Concord
‘We honor your death’ – Arranging services for those who die while homeless in Concord

Sports

Boys’ Lacrosse: Bean reaches milestone in Coe-Brown win over Bow in heavy hitters matchup, 13-3
Seven different players scored for Coe-Brown, including senior attacker Gil Bean who notched his 100th point of the season, in a 13-3 Division III boys’ lacrosse win over Bow on Tuesday.
 High schools: Hillsboro-Deering sweeps Hopkinton; Tuesday’s baseball, softball, lacrosse and tournament tennis
High schools: Hillsboro-Deering sweeps Hopkinton; Tuesday’s baseball, softball, lacrosse and tournament tennis High schools: Concord softball falls on Senior Day; Stark, Brady baseball win on Memorial Day
High schools: Concord softball falls on Senior Day; Stark, Brady baseball win on Memorial Day Track & field: Belmont’s Lacasse, Takantjas win four events each to lead Red Raiders to Wilderness League Championship title
Track & field: Belmont’s Lacasse, Takantjas win four events each to lead Red Raiders to Wilderness League Championship title High schools: Final regular season track and tennis results; plus weekend baseball, softball and lacrosse
High schools: Final regular season track and tennis results; plus weekend baseball, softball and lacrosseOpinion

Opinion: How dark can it get?
Jonathan P. Baird lives in Wilmot.
 Opinion: Unfair taxes, unfair schools: The New Hampshire way
Opinion: Unfair taxes, unfair schools: The New Hampshire way
 Opinion: In the fight to stop sexual violence, can polio hold the solutions?
Opinion: In the fight to stop sexual violence, can polio hold the solutions?
 Opinion: Where are the permanent solutions for a more stable budget?
Opinion: Where are the permanent solutions for a more stable budget?
 Opinion: My memories of Vietnam 50 years later
Opinion: My memories of Vietnam 50 years later

Your Daily Puzzles
An approachable redesign to a classic. Explore our "hints."
A quick daily flip. Finally, someone cracked the code on digital jigsaw puzzles.
Chess but with chaos: Every day is a unique, wacky board.
Word search but as a strategy game. Clearing the board feels really good.
Align the letters in just the right way to spell a word. And then more words.
Politics

New Hampshire school phone ban could be among strictest in the country
When Gov. Kelly Ayotte called on the state legislature to pass a school phone ban in January, the pivotal question wasn’t whether the widely popular policy would pass but how far it would go.
 Concord became a Housing Champion. Now, state lawmakers could eliminate the funding.
Concord became a Housing Champion. Now, state lawmakers could eliminate the funding. ‘A wild accusation’: House votes to nix Child Advocate after Rep. suggests legislative interference
‘A wild accusation’: House votes to nix Child Advocate after Rep. suggests legislative interference  Sununu decides he won’t run for Senate despite praise from Trump
Sununu decides he won’t run for Senate despite praise from Trump
 Town elections offer preview of citizenship voting rules being considered nationwide
Town elections offer preview of citizenship voting rules being considered nationwidee-Edition
Arts & Life

Artist Spotlight: Brittany Batchelder
With creativity abounding in the community around us, The Concord Insider, in collaboration with Concord Arts Market, highlights local artists on a regular basis.
 Young Professional of the Month Katie Duncan shares about creativity, community, connection
Young Professional of the Month Katie Duncan shares about creativity, community, connection Tiny Tapestry sale at Red River Theaters raising money for Concord Coalition to End Homelessness
Tiny Tapestry sale at Red River Theaters raising money for Concord Coalition to End Homelessness Bowling for a cause: Angelman Syndrome Fundraiser coming to Boutwell’s
Bowling for a cause: Angelman Syndrome Fundraiser coming to Boutwell’s
 Beautify Allenstown hosting community cleanup day
Beautify Allenstown hosting community cleanup day
Obituaries
 Alexander William Saltmarsh
Alexander William Saltmarsh
Bow, NH - It is with profound sadness that we announce the passing of Alexander William Saltmarsh, a lifelong resident of Bow, New Hampshire, who died peacefully at the family home on May 19, 2025, at the age of 79. Born on January 31, ... remainder of obit for Alexander William Saltmarsh
 Alexander William Saltmarsh
Alexander William Saltmarsh
Bow, NH - It is with profound sadness that we announce the passing of Alexander William Saltmarsh, a lifelong resident of Bow, New Hampshire, who died peacefully at the family home on May 19, 2025, at the age of 79. Born on January 31, ... remainder of obit for Alexander William Saltmarsh
 Francis Marcellino Jr.
Francis Marcellino Jr.
Francis "Frank" Marcellino Jr. Concord, NH - Memorial Visiting Hours will be held on Friday, June 6th from 4 to 7 PM at the Waters Funeral Home, 50 South Main Street, Concord for Francis "Frank" Marcellino Jr., age 88 of Concord, NH, who ... remainder of obit for Francis Marcellino Jr.
 A. Scott Wiren
A. Scott Wiren
Loudon, NH - Mr. Scott Wiren, 83, of Loudon, passed away peacefully in the care of the Granite VNA Hospice House on May 26, 2025 after a long period of declining health. Born in Concord, Scott was the eldest son of the late Allen and D... remainder of obit for A. Scott Wiren

